The senses 1: hearing, balance and common pathologies of the ear - Nursing Times
The first in a series of articles on the senses examines the nature of hearing and balance (equilibrium). This is a Self-assessment article and comes with a self-assessment test
NT Self-assessment articles offer bitesize CPD and are accompanied by multiple-choice assessments with feedback. Test yourself on this article or click here to choose other subjects from the Self-assessment archive.
Abstract
This series of articles will examine the anatomy and physiology associated with the five major human senses. In this first article, we examine the nature of hearing and balance (equilibrium). The ability to detect sound and balance the human body is reliant on highly specialised sensory organs located in the inner ear. The cochlea is where the organ of Corti is located, which is responsible for detecting sound waves; the vestibule and semicircular canals detect physical movement and are responsible for the sense of balance.
Citation: Knight J et al (2022) The senses 1: hearing, balance and common pathologies of the ear. Nursing Times [online]; 118; 10.
Authors: John Knight is associate professor; Zubeyde Bayram-Weston is senior lecturer; Maria Andrade-Sienz is honorary associate professor; all at School of Health and Social Care, Swansea University.
Introduction
Sound waves transmitted through the air can be thought of as changes in air pressure. Audio communication between humans most commonly involves speaking.
When a person speaks, air is passed through the vocal cords in a highly coordinated manner. This causes the vocal cords to vibrate and generate sound waves, which are transmitted through the atmosphere, where they can be perceived by individuals in the vicinity. If the speaker shouts (increases their volume), the amplitude of the sound waves increases; if they speak more quietly, or whisper, the amplitude of the sound waves decreases. The speaker can also change the pitch of their voice by tightening or loosening their vocal cords. If the vocal cords are tightened, the pitch of the voice will increase along with the frequency of the sound waves; conversely, if the vocal cords are loosened, the pitch of the voice and frequency of the sound waves will be lower (Fig 1).

During speech, the pitch and volume of the voice is continually varied so words can be effectively communicated and emphasis be placed at key points in the conversation. Humans are also very visual communicators, with effective communication involving many non-verbal signals, such as movement of the lips and other facial expressions. In addition to facial expressions, posture, bodily movement and gesticulations, particularly using the arms and hands, are all important visual cues.
Anatomy of the ear
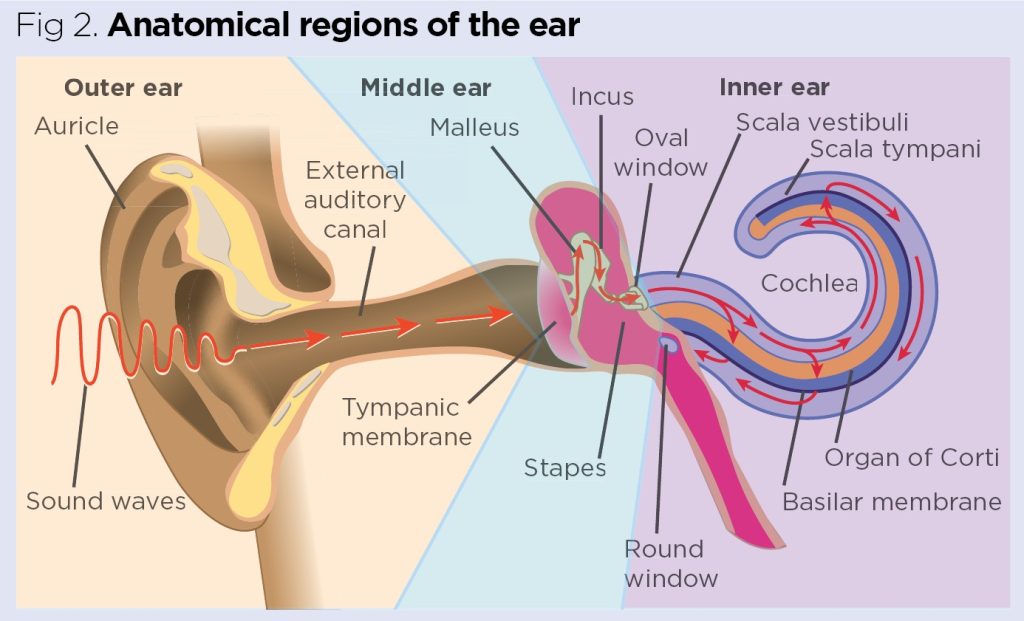
The human ear has three major regions: the outer (or external) ear, the middle ear and the inner ear (Fig 2).
The outer ear
Also known as the external ear, the outer ear consists of the pinna (auricle) and the ear canal (external auditory meatus). The pinna is a flexible structure, which is mainly composed of elastic cartilage covered by skin. Its primary function is to collect sound waves from the atmosphere; these are then directed into the ear canal, which passes into the temporal bone at the side of the skull.
The auditory cartilage, forming the pinna, extends into the first third of the ear canal, where it acts to support and maintain its structure. Common variations in the outer ear include protruding ears, macrotia (abnormal enlargement of the pinna) and microtia (the pinna is underdeveloped and much smaller than normal). These variations in pinna structure can either be bilateral or unilateral (Deep et al, 2016). The adult ear canal is typically around 9.5mm in height, 6.5mm in width and 25mm in length, and terminates at the tympanic membrane (eardrum).
The skin of the ear canal has hairs (particularly near its entrance), which help to prevent the entry of dust and debris. This skin contains many active sebaceous and ceruminous glands, whose secretions contribute to the production of earwax (Felfela, 2017). The epithelial cells of the skin that line the ear canal naturally migrate from the proximity of the tympanic membrane towards the ear opening; this movement can be visualised as a slow conveyor belt, which naturally moves dead skin cells, shed through desquamation, through the ear canal.
Earwax
During the transport process outlined above there is a mixing of the secretions of the ceruminous glands, sebaceous glands, shed skin cells, and atmospheric dust and debris. This complex mixture is a thick, oily, brownish substance that is commonly referred to as earwax or cerumen. The conveyor mechanism ensures earwax is gradually transported out of the ear, with movement further enhanced by the jaw movements associated with chewing and speaking (Horton et al, 2020). For this reason, many health professionals refer to the ears as being 'self-cleaning'.
This transport mechanism can be interrupted, however, by inserting cotton buds, hairpins or other implements into the ear; the result is that earwax can build up and become impacted close to the tympanic membrane. Accumulation of excess wax can lead to conductive hearing loss, tinnitus, chronic coughs and dizziness; this often necessitates interventions involving the use of cerumenolytic agents to soften the wax, followed by irrigation and cleaning procedures. It has been estimated that around 2.4 million ear irrigations are carried out each year in England and Wales (Rodríguez et al, 2022).
Earwax is composed largely of:
- Desquamated cells (60%);
- Saturated and unsaturated fatty acids (12-20%);
- Cholesterol (6-10%).
It is known to have antimicrobial properties, which have been shown to be effective against a variety of bacteria, including species of pseudomonas, staphylococcus, escherichia, and proteus (Naz, 2020). Despite the antimicrobial activity present in earwax, the outer ear is home to a diverse community of micro-organisms. The microbiome of a healthy ear canal is predominantly composed of bacteria that have adapted to this unique environment, including Staphylococcus auricularis, Propionibacterium acnes, Alloiococcus otitis and Turicella otitidis (Sjövall et al, 2021).
Otitis externa (swimmer's ear)
Inflammation of the ear canal is referred to as otitis externa and is most often caused by bacterial infection, particularly by Pseudomonas aeruginosa and Staphylococcus aureus. This condition is often referred to as 'swimmer's ear', because swimming in communal pools is recognised as a major risk factor (Medina-Blasini and Sharman, 2022).
Otitis externa is characterised by painful inflammation and itching (pruritus), and may also be accompanied with fever (pyrexia). Occasionally, the infection may spread outwards to affect the pinna. It has been estimated that 10% of people will develop otitis externa during their lifetime, with the condition usually resolving following the use of topical antibiotic drops; these are often prescribed together with analgesics to relieve pain (Medina-Blasini and Sharman, 2022).
The middle ear
Sound waves travelling along the ear canal cause the tympanic membrane to vibrate. This cone-shaped, pearl grey membrane is the first part of the middle ear and is usually kept under tension (hence the term 'eardrum'). The tympanic membrane is a compound membrane consisting of three distinct layers:
- Outer cutaneous layer (on the side of the ear canal);
- Middle fibrous layer;
- Inner mucosal layer.
This laminar structure provides extra strength, although the tympanic membrane remains fragile with a total thickness of only around 0.1mm (Kim and Shin, 2018).
Vibrations are transferred through the three auditory ossicles – the tiny bones – that span the air-filled middle-ear cavity. The first of the auditory ossicles is the malleus (hammer), which is attached to the inner mucosal surface of the tympanic membrane. Sound waves are transmitted from the malleus to the incus (anvil) and then on to the final of the three ossicles, the stapes (stirrup).
The three ossicles are linked together to form a continuous chain. They are connected to each other by tiny articular synovial joints, which facilitate the incredibly efficient conduction of sound waves. The ossicles also function as levers and amplify the sound as it is conducted through the chamber of the middle ear. The final stapes bone rests in a small aperture at the beginning of the cochlea, termed the oval window (Saha et al, 2017).
As the tympanic membrane is so thin, it is important to make sure the air pressure on both sides is equal. The middle-ear cavity is connected to the back of the pharynx (throat) by a mucous membrane-lined passageway called the Eustachian tube. This usually ensures the atmospheric pressure is equalised on both sides of the tympanic membrane. The Eustachian tube is partially reinforced by cartilage and typically remains in a semi-collapsed state, although it usually opens during chewing, yawning and swallowing (Llewellyn et al, 2014).
When a person has a heavy, productive cold, there is a tendency for the Eustachian tube to become blocked by catarrhal secretions.
This can lead to symptoms such as earache or dizziness but, at ground level, is unlikely to lead to damage to the tympanic membrane. However, blockage of the Eustachian tube when on an aeroplane flight can cause immense pain when the plane is taking off or landing; this is due to sudden changes in atmospheric pressure. This is a common phenomenon when flying and may even occur in the absence of a cold; it is often referred to as 'airplane ear' or 'ear barotrauma' (Bhattacharya et al, 2019).
In children, the Eustachian tubes are shorter and smaller, which can make equalising air pressure more difficult (Harkin, 2021). This explains why young children, and especially babies, are prone to barotrauma when flying.
"Exposure to loud sounds, particularly chronic exposure, can lead to more rapid noise-induced hearing loss"
Otitis media
The Eustachian tubes can also provide a potential route for pathogens from the pharynx to the middle-ear chamber, leading to infection and a painful inflammation termed otitis media. This is particularly common in children, where it often follows viral upper respiratory tract infections, such as a common cold. It has been suggested that viral infections may upset the normal healthy microbial biome of the nose, throat and Eustachian tube, and make infection of the middle ear by aggressive pathogens more likely (Venekamp et al, 2020).
The most common pathogens associated with otitis media are Streptococcus pneumoniae, Haemophilus influenzae and Moraxella catarrhalis. A build-up of inflammatory exudate in the middle-ear chamber typically increases the pressure within and stretches the tympanic membrane; this can lead to intense pain and chronic earache. There is also the potential for tympanic rupture, with leakage of purulent exudates into the auditory canal.
Most cases of otitis media are acute and self-limiting, usually resolving in seven to eight days. Analgesics are used to manage pain and antibiotics may be prescribed, particularly if there is chronic infection, fever or risk of the infection spreading (Venekamp et al, 2020).
The inner ear
The inner ear consists of a group of interconnected, fluid-filled chambers located in the temporal bones of the skull. These are collectively known as the bony labyrinth. In the bony labyrinth are membrane-bound, fluid-filled ducts, which are referred to as the membranous labyrinth.
The inner ear consists of three major regions, each with distinct functions:
- Cochlea – hearing;
- Vestibule – static equilibrium;
- Semicircular canals – dynamic equilibrium.
Internal structure of the cochlea
The cochlea (Fig 2 and Fig 3) is a snail-shaped, spiral organ typically consisting of between 2.5-2.75 turns with a total length (unwound) of around 29.5-32mm (Vaid and Vaid, 2014).

Internally, the cochlea consists of three fluid-filled ducts (Fig 3a). The upper duct is called the vestibular canal (scala vestibuli); this begins at the oval window (Fig 2) and runs the length of the cochlea. At the apex of the cochlea is a tiny opening called the helicotrema (Fig 2); this connects the vestibular canal with the tympanic canal (scala tympani), which runs in parallel beneath. Both the vestibular and tympanic canals are filled with an aqueous fluid called perilymph.
Running through the middle of the cochlea, in between the vestibular and tympanic canals, is the cochlear duct. This is entirely membrane bound and filled with a fluid called endolymph. The cochlear duct contains the organ of Corti (Fig 3). This is the sensory structure of the ear responsible for detecting sound and functions by transducing sound waves into nerve impulses (action potentials) that are then relayed to the brain.
The organ of Corti contains sensory 'hair cells' that reside on a basilar membrane in the cochlear duct. The 'hairs' of these cells are specialised cell membrane extensions termed stereocilia; they are in close proximity to, and almost touching, a thicker membrane called the tectorial membrane, which resides above (Casale et al, 2022; VanPutte et al, 2017).
Detection of sound in the cochlea
Sound waves pass through the auditory ossicles and are transmitted to the oval window of the cochlea through the stapes (Fig 2). The footplate of the stapes can be visualised as having a piston-like movement as it transmits the physical vibrations of the ossicles to the oval window. Sound waves move more efficiently through fluid and are rapidly conducted through the perilymph along the entire length of the vestibular canal. The helicotrema facilitates transmission of sound to the tympanic canal beneath, before the sound waves exit the cochlea through the round window (Fig 2).
Fluid disturbances created in the perilymph are continually transmitted to the endolymph in the cochlear duct; this causes vibrations in the basilar membrane, which moves in harmony with the conducted sound waves. These movements cause deformation of stereocilia as they press against the thicker tectorial membrane above; this initiates the generation of nerve impulses (Casale et al, 2022; VanPutte et al, 2017).
The auditory cortex
Nerve impulses generated by the organ of Corti are transmitted through the cochlear branch of the vestibulocochlear nerve (cranial nerve VIII). The auditory cortices of the brain are located in the temporal lobes of the cerebral hemispheres; here, these signals are decoded, allowing the conscious perception of sound (Yoo et al, 2021).
The acoustic reflex
The stapes is connected to the temporal bone by the stapedius muscle; this is the smallest skeletal muscle in the human body. In response to loud sounds the stapedius contracts, pulling the footplate of the stapes slightly away from the oval window, thereby reducing the transmission of damaging high-amplitude (high-volume) sound waves into the delicate cochlea. This mechanism is referred to as the acoustic or stapedius reflex and, although it is an effective damage-limiting mechanism, it can take up to 100 milliseconds (one tenth of a second) to initiate. This means that sudden, very loud sounds can still inflict significant damage to the inner ear (Bell, 2017).
Another small skeletal muscle called the tensor tympani connects the malleus to the cartilaginous portion of the Eustachian tube. This muscle also plays a role in the acoustic reflex by tensing and pulling on the malleus, thereby tightening the tympanic membrane; it is also thought to dampen the sound generated when chewing, swallowing and yawning (Noreña et al, 2018).
Hearing loss and tinnitus
Hearing acuity tends to diminish gradually with age. This phenomenon is termed presbycusis and occurs as a result of age-related changes in the ear; this often necessitates the use of hearing aids in later life (Knight et al, 2017).
Exposure to loud sounds, particularly chronic exposure, can lead to more rapid noise-induced hearing loss. This is commonly seen in people with occupations that involve being continually exposed to loud sounds, such as workers using pneumatic drills, chainsaws or heavy machinery, and military personnel exposed to loud gunfire and explosions.
Long-term exposure to loud noise can directly damage nerve cells and disrupt the structure of the delicate hair cells in the organ of Corti. Exposure to sounds of around 85 decibels (approximately equivalent to the sound of a train passing close by) over prolonged periods of time can be damaging to hearing, while sounds exceeding 89 decibels for more than five hours a week have been associated with permanent hearing loss (Wang et al, 2020).
Noise-induced hearing loss is frequently associated with tinnitus. This is a common condition in which intrusive ringing, humming, buzzing or other sounds are perceived that are not actually present in the outside world. Research indicates that, in many patients, tinnitus is related to the physical damage caused to the cochlea as a result of being exposed to excessive noise (Wang et al, 2020).
Sense of balance (equilibrium)
Static equilibrium
Static equilibrium can be thought of as the ability to balance the body when it is at rest and not moving. It provides information to the brain about basic body position in relation to gravity, for example, leaning to the left or right. The vestibule is the structure primarily dedicated to static equilibrium; it consists of two hollow regions, termed the utricle and saccule, which are filled with endolymph. Like the cochlea, these regions contain hair cells but, here, their stereocilia are embedded in a gelatinous matrix (resembling a slab of jelly), which is weighted with small calcium-rich crystals termed otoconia (Fig 4).

During changes in position, such as tilting the head, gravity acts on the gelatinous matrix causing it to shift and bend the embedded stereocilia. This leads to the generation of nerve impulses (Jones et al, 2009).
Dynamic equilibrium
Dynamic equilibrium is the ability to balance the body during movement. It is primarily reliant on the three semicircular canals, which are positioned to detect movement in the three planes of three-dimensional space. The distal end of each semicircular canal is expanded into a bulbous cavity termed an ampulla (Fig 4). In each of the ampullae are populations of hair cells, which have their stereocilia embedded in a triangular-shaped gelatinous mass termed a cupula. The semicircular canals are filled with endolymph, which moves in response to physical movement, for example, pirouetting on a dance floor. During such movements the shifting endolymph presses against and moves the cupula, distorting the stereocilia of the hair cells, thereby initiating the generation of nerve impulses (Rabbitt, 2019).
Neural pathways involved in equilibrium
Nerve impulses generated by the utricle, saccule and semicircular canals are relayed along the vestibulocochlear nerve to the vestibular nuclei; these are located between the medulla oblongata and the pons of the brainstem. The vestibular nuclei integrate this information and relay it to the cerebellum, which is a key area of the brain dedicated to balance and coordination. Information is also relayed to the cerebral hemispheres to allow conscious perception of position and movement (Martini et al, 2018).
Benign positional vertigo (BPV)
BPV is the most common cause of vertigo; it is precipitated by detachment of the otoconia crystals from the gelatinous matrices of the utricles and saccules. These free crystal particles can then become mobile in the endolymph of the vestibular system and enter the semicircular canals, interfering with their ability to accurately detect physical movement.
In many cases, BPV can be effectively resolved using particle-repositioning manoeuvres, such as the Epley manoeuvre. These rely on a trained health practitioner accurately manipulating the patient's head to reposition the dislodged crystals back into their correct positions in the utricle and saccule (Palmeri and Kumar, 2022).
Conclusion
This article has examined the anatomy, physiology and common pathologies of the ear, focusing on the role of the ear in hearing and balance.
Key points
- Hearing is one of five major senses, with the ear also being responsible for maintaining balance
- The human ear has three major regions: outer, middle and inner
- Specialised sensory organs in the ear enable sound to be detected, with sound waves transduced into nerve impulses relayed to the brain
- Dynamic equilibrium is the ability to balance during movement, with information relayed from the inner ear to the cerebellum
- Exposure to sounds of >89 decibels for more than five hours a week has been associated with permanent
hearing loss

- Test your knowledge with Nursing Times Self-assessment after reading this article. If you score 80% or more, you will receive a personalised certificate that you can download and store in your NT Portfolio as CPD or revalidation evidence.
- Take the Nursing Times Self-assessment for this article
Bell A (2017) A fast, "zero synapse" acoustic reflex: middle ear muscles physically sense eardrum vibration. Journal of Hearing Science; 7: 4, 33-44.
Bhattacharya S et al (2019) "Airplane ear": a neglected yet preventable problem. AIMS Public Health; 6: 3, 320-325.
Casale J et al (2022) Physiology, Cochlear Function. StatPearls [Internet]. StatPearls Publishing.
Deep A et al (2016) Ear. In: Tubbs RS et al (eds) Bergman's Comprehensive Encyclopedia of Human Anatomic Variation. Wiley-Blackwell.
Felfela GMW (2017) Ear anatomy. Global Journal of Otolaryngology; 4: 1, 555630.
Harkin H (2021) The structure and function of the ear and its role in hearing and balance. Nursing Times [online]; 117: 4, 56-59.
Horton GA et al (2020) Cerumen management: an updated clinical review and evidence-based approach for primary care physicians. Journal of Primary Care and Community Health; 11: 2150132720904181.
Jones SM et al (2009) Anatomical and physiological considerations in vestibular dysfunction and compensation. Seminars in Hearing; 30: 4, 231-241.
Kim C-H, Shin JE (2018) Hemorrhage within the tympanic membrane without perforation. Journal of Otolaryngology – Head and Neck Surgery; 47: 1, 66.
Knight J et al (2017) Anatomy and physiology of ageing 6: the eyes and ears. Nursing Times [online]; 113: 7, 39-42.
Llewellyn A et al (2014) Interventions for adult Eustachian tube dysfunction: a systematic review. Health Technology Assessment; 18: 46, 1–180.
Martini FH et al (2018) Fundamentals of Anatomy and Physiology. Pearson.
Medina-Blasini Y, Sharman T (2022) Otitis Externa. StatPearls [Internet]. StatPearls Publishing.
Naz I (2020) The assessment of antimicrobial activity of cerumen (earwax) and antibiotics against pathogenic bacteria isolated from ear pus samples. Microbiology Research; 11: 8565.
Noreña A et al (2018) An integrative model accounting for the symptom cluster triggered after an acoustic shock. Trends in Hearing; 22: 2331216518801725.
Palmeri R, Kumar A (2022) Benign Paroxysmal Positional Vertigo. StatPearls [Internet]. StatPearls Publishing.
Rabbitt RD (2019) Semicircular canal biomechanics in health and disease. Journal of Neurophysiology; 121: 3, 732-755.
Rodríguez R et al (2022) Mechanism cleaning of the ear canal. Inventions; 7: 20.
Saha R et al (2017) Morphological variations of middle ear ossicles and its clinical implications. Journal of Clinical and Diagnostic Research; 11: 1, AC01-AC04.
Sjövall A et al (2021) Microbiome of the healthy external auditory canal. Otology and Neurotology; 42: 5, e609-e614.
Vaid S, Vaid N (2014) Imaging for cochlear implantation: structuring a clinically relevant report. Clinical Radiology; 69: 7, e9-e24.
VanPutte CL et al (2017) Seeley's Anatomy and Physiology. McGraw-Hill.
Venekamp RP et al (2020) Acute middle ear infection (acute otitis media) in children. BMJ; 371: m4238.
Wang T-C et al (2020) Noise induced hearing loss and tinnitus: new research developments and remaining gaps in disease assessment, treatment, and prevention. Brain Sciences; 10: 10, 732.
Yoo S-H et al (2021) Decoding multiple sound-categories in the auditory cortex by neural networks: an fNIRS study. Frontiers in Human Neuroscience; 15: 636191.
Don't miss more great clinical content from Nursing Times
NT Bitesize learning videos – helping you to organise learning to fit in with your schedule
Clinical zones – keep up to date with articles in your clinical subject or nursing role/setting
CPD zone – user-friendly online learning units on fundamental aspects of nursing
Journal Club – clinical articles with discussion handouts for participatory CPD
Practical Procedures – 'how to' guides and teaching materials for clinical procedures
Self-assessment – clinical articles with linked online assessments for bitesize CPD
Systems of Life – applied anatomy and physiology to support your practice


Comments
Post a Comment